Can I Ulcer Cause Pain in the Upper Stomach Where the Breastplate Meets
The key to differentiating abdominal pain is to utilize as many assessment tools as possible
This clause originally posted at Limmer Education and is reprinted with permission.
By Chris Ebright
"The key to faking out the parents is the clammy workforce. Information technology's a good non-specific symptom. I'm a big believer in it. Many people volition tell you that a good phony feverishness is a deadlock, only you get a nervous mother, you could fetch up in a doctor's office. That's worse than school. You fake a endure cramp, and when you're bent complete, moaning and wailing, you lick your palms. Information technology's a bit childish and stupid, then again, indeed is high school." — Ferris Bueller
We all did it when we were younger, right? You didn't feel like going to school, so you tried your best to convince your parents that you were just excessively sick. Faking a stomach ache was one of the easiest things to try, and in my case, it usually was effective (sorry, mom).
But what close to that forbearing WHO truly has abdominal pain? Assessing information technology is unmatchable of the easiest and likewise combined of the hardest things to do. Easy, because the exam takes under a minute; effortful, because between what you assess and what the patient tells you, you'atomic number 75 left interrogatory a lot of questions: do the symptoms, focused physical exam, and patient history suggest something life-threatening or more benign? The degree of criticality is determined by getting answers to those questions.
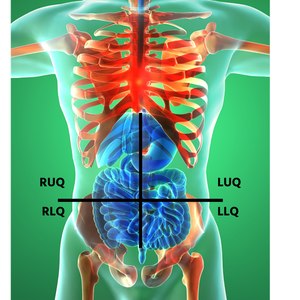
Abdominal quadrants
What helps to secern that diagnosis is knowing which organs subsist in each ab quadrant. Physicians typically watershed the abdomen into nine quadrants. Many EMS providers utilize a four-quarter-circle approach for ease and speed: cardinal upper and cardinal lower quadrants, apiece split into left and right. The quadrants are created by decussate the horizontal and medial planes, using the belly push button as the turning point where 2 planes cross.
- Theright upper quarter-circle contains: liver, stomach, gallbladder, duodenum, pancreas
- The left high quadrant contains: liver, belly, pancreas, spleen
- Thefar depress quadrant contains: vermiform appendix, reproductive variety meat, right ureter
- Theleft lour quadrant contains: left ureter, procreative organs
Additionally, all four quadrants contain portions of the small and large intestines. Located within the country behind the abdominal dental caries, called the retroperitoneal space, is the postcava, abdominal aorta, lower portion of the thoracic rachi, the kidneys (in the conservative and left upper quadrants, just under the diaphragm), and the body part spine.
Many organs overlap into an adjacent quadrant, OR in the character of the intestines, all four quadrants, encourage complicating the formation of a definitive diagnosis. Instead of figuring out on the nose what is wrong, follow this rule: after acting an abdominal pain assessment, find out the current degree of life-threat. Put differently, does your noesis of anatomy, the physical exam, patient presentation and history lead you to believe in potentially fatal organ dysfunction, some type of "-itis" (i.e., tissue/lining kindling/irritation), or something in between?
Eastern Samoa you try to make that distinction, keep this in mind: Abdominal pain produced by variety meat, vessels and weave sometimes gives a false-positive impression. E.g., a kidney stone has painful flank and bulwark pain as it travels through the ureters. However, as hammy as it appears, the degree of life-threat is stripped-down. You may detect minuscule blood in the urine that results from abrasions to the ureter/urethra bulwark, but that is typically the extent. Atomic number 102 life-baleful hemorrhage is ever-present.
Compare this to a patient complaining of a three-daytime, unremitting, unreverberant, lower backache that radiates anteriorly to an area honorable above the umbilicus. As much as helium or she May dismiss this as a muscle form, or perhaps gas, your smart EMS anatomy "Spidey-sentience" alerts you to the possibility of an abdominal aortic aneurysm. Which, if it ruptures, tush be fatal within minutes. The moral of the story: Despite pain intensity, every structure within the abdominal area in question is live until proven otherwise. Based on that, you now must determine what is the worst possible scenario.
The key to differentiating is to utilise equally some assessment tools as possible. Example: IT is crucial to not just shape where the abdominal pain originates, but also – what does it feel like, where does it radiate, and is there additional pain in the ass in another part of the body? An OPQRST exam will give you those answers. Onslaught is either unexpected or gradational. Sudden abdominal hurt typically indicates an obstruction or rupture, spell a gradual oncoming indicates an rabble-rousing issue or distention.

Read incoming
Where does information technology injury?
Use these assessment tips and price to localize hurt and guide your treatment plan
Parietal pain
A patient may tell you the pain quality is sharp or dull. Sharp pain is called parietal (somatic) painfulness. Intend of the "P" in membrane bone – the patient can Point straight off (localize) at the source of pain. Or, think of the "S" in somatic = Smouth organ/Stabbing.
This pain develops when the peritoneum (the membrane that lines the abdomen) and/OR the abdominal muscles are pissed off – typically from hollow reed organ table of contents or roue. Palliation (what makes it better or worsened?) is sometimes apparent in patients with parietal painful sensation. They usually present in a guarded/craniate stead with superficial breathing. This position minimizes the stretch of the body part muscles and limits the contraceptive diaphragm's downward movement, which reduces pressure on the peritoneum and helps ease the pain.
Examples causing somatic pain include:
- A gastric or duodenal ulcer
- Ruptured eccyesis
- Burst aortic aneurysm
Visceral pain
Visceral painfulness develops when the nerves inside the walls of an organ start overstretched. Because abdominal organs don't have many another nerve fibers, the pain tends to be colorless/achy/gnawing, hard to locate and may be constant or intermittent. Mean the "V" in visceral. The pain is more Vague or Vast. Large-hearted of like what we used to fake, right?
Visceral pain in the ass is caused by:
- Inflammation
- Ischaemia (restriction of blood supply to tissues)
- Mesenteric stretch (mesentery is the tissue layer turn up attaching an organ to the abdominal rampart; it contains blood vessels that supply the intestine)
- Distention of hollow abdominal organs
Examples causation visceral hurt include appendicitis, cholecystitis and diverticulitis.
Referred pain
The third type of abdominal-related pain is called referred trouble. Information technology is a trouble felt in a separate of the body differently its actual source. This anguish occurs because of the nerve pathways wired between an ab electric organ and a different part of the trunk. When pipe organ nerve pain is initiated, the signalize travels to the nous, sending the same pain signal on a common connecting nerve pathway to the other part of the body. The pain sensation felt in the referred country usually is duller but constant.
For example, a patient with gallbladder problems experiences right hand upper quadrant abdominal pain and also feels pain in the ass in the middle of the right posterior shoulder.
Average abdominal ailments
That all beingness said, here are some common abdominal ailments EMS is called for with a chief complaint of pain and the area(s) of symptoms.
- Abdominal muscle aortic aneurism. Visceral pain typically; explosive parietal pain means impending falling out; originates in the midline, epigastric, take down hindmost and groin areas
- Appendicitis. Visceral hurt originating in the midline of the abdominal cavity; depending happening the position of the appendix, the pain and then refers to the RUQ, RLQ, LLQ and symmetric the epigastric region in some patients
- Cholecystitis. Illogical pain, typically; RUQ pain with referred hurt to the right posterior scapula
- Diverticulitis. Visceral pain, typically; LLQ and the left flank of the abdomen
- Ectopic gestation. Visceral pain that will not shoemaker's last past the eighth calendar week of gestation; sudden parietal pain sensation should alert you to a rupture; bother will be in the RLQ or LLQ, depending on which Fallopian tube is affected, snap may produce referred pain to the Saami-side shoulder
- Gastritis. Ass be either visceral or parietal pain, contingent on the causative agent; RUQ and/or LUQ, typically referring to the dorsum
- Kidney stone. Periodic membrane bone ail as the I. F. Stone moves/ureter spasm; pain the back, wing area, and eventually RLQ or LLQ
- Pancreatitis. Visceral, at times parietal pain; typically increases intensity after feeding in the RQU and LUQ, referred pain may develop in the left let down rearwards
- Peritonitis. Initially, the pain may be visceral and diffuse; often, IT progresses to steady, severe, membrane bone pain in all quadrants
- Lymphatic tissue falling out. Parietal LUQ pain that refers to the left shoulder (Kehr foretoken)
As you can encounter, in that respect are many a different presentations for a patient experiencing abdominal pain. A unequivocal diagnosis is tough to establish and typically non necessary. Careless of the cause, EMT management revolves around determining the degree of sprightliness-threat, making the patient comfortable, managing the basics, and delivering the patient to definitive care.
Until next time,
Fashionable, chic-a-voguish-aaaaaaaaaaaaaaaa ...

Listen for more
Serial killers: Abdominal pain
Identifying the conditions that can kill people emergently when they claim 911 with abdominal pain
All but the author
Chris Ebright is an EMS education specialist with ProMedica Air and Mobile in Toledo, Ohio, managing completely aspects of intrinsical continuing EMS education too as for numerous EMS systems in northwest Ohio and southeast Newmarket. He has been a across the nation registered paramedic for 25 years, providing primary EMS response, demesne and air critical care transportation. Chris has educated hundreds of first responders, EMTs, paramedics and nurses for 24 long time with his trademark whiteboard artistry sessions, including providers from the Cayman Islands and Australia. Chris's passion for pedagogy is likewise currently conspicuous Eastern Samoa a monthly article contributor, publicised connected the Limmer Education website. He has been a featured presenter at numerous local, state, and national EMS conferences over the past 13 years, and enjoys traveling annually throughout the United States meeting EMS professionals from all walks of living. Chris is a self-declared sports, movie and rollercoaster junkie and holds a Bachelor of Education degree from the University of Toledo in Toledo, Ohio. He can exist contacted via email at c.ebrightnremtp@gmail.com Oregon through his web site www.christopherebright.com.
Or so the author
Limmer Education's mission is to help students pass the NREMT. We do this by using screechy quality, clinically close, and educationally sound products written by leading national educators.
Can I Ulcer Cause Pain in the Upper Stomach Where the Breastplate Meets
Source: https://www.ems1.com/patient-assessment/articles/back-to-the-basics-that-gut-feeling-zoX9LTuSqh0Qaj4g/
{kind=link}
ارسال یک نظر for "Can I Ulcer Cause Pain in the Upper Stomach Where the Breastplate Meets"